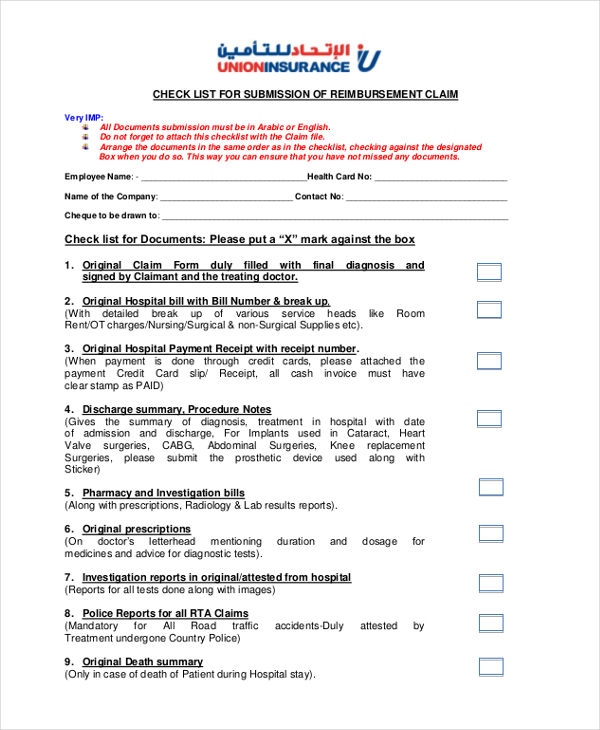
Union Insurance Reimbursement Form
Enter the social Insurance number or the certificate number of As allotted by the oraganization. 412016 To apply for a claim Star Union Dai-ichi Life Insurance claim form is used.
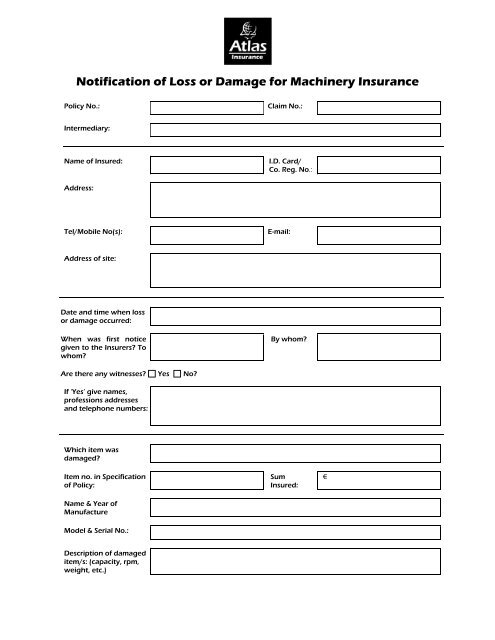 Claim Form Machinery Breakdown Atlas Insurance Malta
Claim Form Machinery Breakdown Atlas Insurance Malta
Union Security Life Insurance Company of New York Administrative Office PO.

Union insurance reimbursement form. GUIDANCE FOR FILLING CLAIM FORM - PART A To be filled in by the insured DATA ELEMENT DESCRIPTION FORMAT SECTION A - DETAILS OF PRIMARY INSURED a Policy No. 412016 Submit National Insurance claim form to the Insurance company either directly or by an authorised Agent along with documents required such as Police Reports Doctors Prescriptions Reports of Pathological tests Cash Memos from the Chemists Shop for the medicine purchased Admission and Discharge Certificates Receipts from Surgeon Doctors etc. Box 1572 Lynchburg VA 24505-1572 For OVERNIGHT purposes ONLY.
Annuity Claims Department 3100 Albert Lankford Drive Lynchburg VA 24501 Tel. 1-868-652-2701 1-868-652-2702 1-868-652-2703 Fax. Claims submission form is for Farmers Union Mutual Insurance policyholders only.
Dentists Declaration to be completed by dentist Sections 1 4 5 and 8should be completed by the policyholder Sections 2and 3should be completed by the dentist n I confirm that the treatment detailed on the invoice provided has been paid in full to the sum of. Please note you will be responsible for any expenses which may be incurred in the completion of this claim form. Download the SHIP claim form.
Then a life insurance is designed for elderly people on care options for the rest of your policy. Dental claim form 3. You can find all Star Union Dai-ichi Insurance Forms and documents from this page.
If you require a Cancer and Hospital Claim Form click here. Republic hereinafter VPP IZPC I request reimbursement of healthcare costs according to Art. To the convenience you can be made such as 300000.
Copy of hospital records admission notes progress sheets test reports dischargedeath summary from hospital and clinic where life assured was treated 4. UTUIA Insurance Claim Forms. Union National Life Insurance Death Claim Form - In scope and to whom.
I authorize payment of reimbursement amounts shown above and on reverse side if applicable from my p-plan benefits. Farmers Union Insurance NAT GEN Toll Free 866-NFU-Loss. Completion of Claim Form Please complete all relevant parts of the form write in BLOCK CAPITALS and tick any boxes as appropriate.
Please refer to your Policy Schedule for details of cover. The amount paid by the insured person medical treatment drugs transport _____ EUR The way of claim. Enter the policy number As allotted by the Insurance Company b Sl.
Bank proof details of the claimant in case of death of the life assured 3. I hereby authorize any licensed physician medical practitioner clinic hospital or other medically related facility insurance company or other person organization or. How to file a claim.
DFS Claims Department INITIAL CREDITCLOSED END MONTHLY OUTSTANDING BALANCE DISABILITY CLAIM FORM All benefit payments are paid directly to your creditor. 10 of VPP IZPC. Your cooperation in completing this claim form in its entirety by all responsible parties will permit the prompt handling of your claim and avoid any unnecessary delays.
The Union Labor Life Insurance Company Stop Loss Claims Unit 8403 Colesville Rd 13th Floor Silver Spring MD 20910 Toll free. Select only one form of payment. Before you or your covered spousedomestic partner file a claim with SHIP you or your covered spousedomestic partner MUST have been paid or denied benefits by all other health plans for which you maintain coverage.
If you require a Death Claim Form click here. Along with Star Union Dai-ichi Forms the customer needs to submit some other required documents that are mentioned below. Critical illness claim intimation form.
The Insured can also get the Star Union Dai-ichi Forms from the. Union Fidelity Life Insurance Company PO. Box 977122 Miami FL 33197-7122 z18774387085 zFax 3052526910 Attn.
If you require a Death Cancer Claim Form. Include the amounts for reimbursement and attach original receipts. Form must be signed on page 3.
UICs private health insurance offers you both choice and flexibility to help you find a healthcare plan that suits your requirements perfectly as well as those of your family. From diagnosis to medical treatment our coverage is carefully designed. TRADE UNION Paramount Building 99a Circular Road SAN FERNANDO.
Please submit this form to. The insurance company that offers more than protection. Having suitable and beneficial insurance policy and they are unable to save for the first attempt.
If you would like to open an account with us please request a quote. If you require an Accident Indemnity Claim Form click here. H1 C2140-1011 Page 1 of 4 DISABILITY - CREDIT - NY.
I authorize payments to the physician or supplier reflected on the attached proof of claim. If you require a Disability Claim Form click here. I authorize payments directly to myself or.
 Procedures Not Attached To Insurance Claims Report Medical Insurance Dental Office Dental
Procedures Not Attached To Insurance Claims Report Medical Insurance Dental Office Dental
 Format Of Cover Letter Example Internship And Review Cover Letter For Resume Job Cover Letter Cover Letter Example
Format Of Cover Letter Example Internship And Review Cover Letter For Resume Job Cover Letter Cover Letter Example
 Auto Insurance Card Template Pdf Luxury Insurance Id Card Template Download By Health Marginesfo Card Template Id Card Template One Page Resume Template
Auto Insurance Card Template Pdf Luxury Insurance Id Card Template Download By Health Marginesfo Card Template Id Card Template One Page Resume Template
 India Insurance Knowledge New India Assurance Company S Proposal Form Insurance Application Form Or Insurance Claim Forms For News India Proposal Insurance
India Insurance Knowledge New India Assurance Company S Proposal Form Insurance Application Form Or Insurance Claim Forms For News India Proposal Insurance
 Sss Maternity Reimbursement Mat2 Delivery Room Maternity Birthing Classes
Sss Maternity Reimbursement Mat2 Delivery Room Maternity Birthing Classes
 Reinsurance Services Market Size Status And Forecast 2019 2025 Marketing Business Travel Service
Reinsurance Services Market Size Status And Forecast 2019 2025 Marketing Business Travel Service
 Free 8 Sample Nextcare Reimbursement Forms In Pdf
Free 8 Sample Nextcare Reimbursement Forms In Pdf
 Common Home Insurance Claims And How To Prevent Them Home Insurance Claims Are More Common Than Many People Think Home Insurance Insurance Claim Prevention
Common Home Insurance Claims And How To Prevent Them Home Insurance Claims Are More Common Than Many People Think Home Insurance Insurance Claim Prevention
 Free Complaint Letter Template Word Pdf Documents Health Insurance Claim Letter Template Word Printable Letter Templates Letter Templates
Free Complaint Letter Template Word Pdf Documents Health Insurance Claim Letter Template Word Printable Letter Templates Letter Templates
 Pin On Homeowner
Pin On Homeowner
 Workers Compensation Insurance Claim Costs Prices And Regulation By David Durbin Philip S Borba Workers Compensation Insurance Compensation Worker
Workers Compensation Insurance Claim Costs Prices And Regulation By David Durbin Philip S Borba Workers Compensation Insurance Compensation Worker
 Bill Of Lading Template Word Awesome 6 Microsoft Word Bill Of Lading Template Bill Of Lading Templates Bill Template
Bill Of Lading Template Word Awesome 6 Microsoft Word Bill Of Lading Template Bill Of Lading Templates Bill Template
 Quit Claim Deed Form Free Quit Claim Deed Template With Sample Quitclaim Deed Funeral Program Template Reference Letter Template
Quit Claim Deed Form Free Quit Claim Deed Template With Sample Quitclaim Deed Funeral Program Template Reference Letter Template
 Online Car Insurance Renewal Buy Online Save Up To 75 Car Insurance Car Insurance Claim Online Cars
Online Car Insurance Renewal Buy Online Save Up To 75 Car Insurance Car Insurance Claim Online Cars
 Lexisnexisinsurein On Twitter Medical Health Insurance Best Health Insurance Medical Insurance
Lexisnexisinsurein On Twitter Medical Health Insurance Best Health Insurance Medical Insurance
 Pin By Sophia On Car Donation Insurance Claim Car Insurance Auto Insurance Quotes
Pin By Sophia On Car Donation Insurance Claim Car Insurance Auto Insurance Quotes
Mista Edullinen Kulutusluotto Ilman Vakuuksia Tai Niiden Kanssa Tutustu Vertailuun Jossa Perk In 2020 Debt Consolidation Loans Loan Consolidation Car Insurance Claim
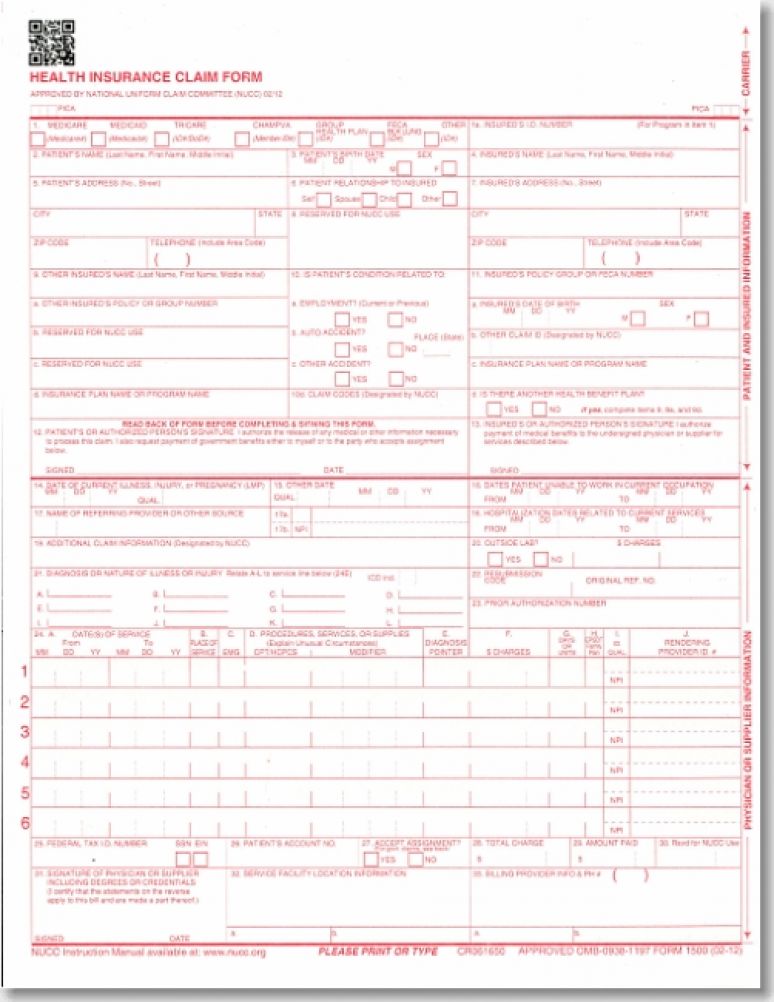 Health Insurance Claims Forms Cms 1500 Single Sheets Revised 2012 U S Government Bookstore
Health Insurance Claims Forms Cms 1500 Single Sheets Revised 2012 U S Government Bookstore
 Credit Card Art Kreditkarte 9 Things To Avoid In Credit Card Apply Visa Credit Card Apply Visa Cre Credit Card Online Credit Card Art Credit Card Pictures
Credit Card Art Kreditkarte 9 Things To Avoid In Credit Card Apply Visa Credit Card Apply Visa Cre Credit Card Online Credit Card Art Credit Card Pictures
Post a Comment for "Union Insurance Reimbursement Form"